
Polymerase chain reaction (PCR) use in the pathology lab differs from research-based PCR in two fundamental ways, namely quality and clinical expertise. These are essential to producing a clinical diagnosis supported by results from a range of tests performed by different branches of ‘the pathology laboratory’. In a research lab, PCR results are often relied on to confirm experimental outcomes. Recognising these differences requires experience in a high-quality pathology lab setting to fully appreciate the absolute need for quality and its ubiquity.

My experience
The many words below are based on 32 years of experience in both research and routine labs, using PCR as a tool to answer a range of questions. PCR is not a simple test – it’s complicated and requires meticulous and ongoing lab cleanliness, the ability to troubleshoot, and distinct dedicated regions for the main parts of the PCR (to be covered by a future post).
Key differences between pathology and research PCR
There are more than I’ve listed, but I’m trying to write a short, sharp post here!
It’s worth noting that during the peak of the COVID-19 pandemic, the World Health Organization had to gently remind new high-throughput PCR adopters, possibly including one or two researchers who had generously offered their research skills, resources and space, to read the damned manual!
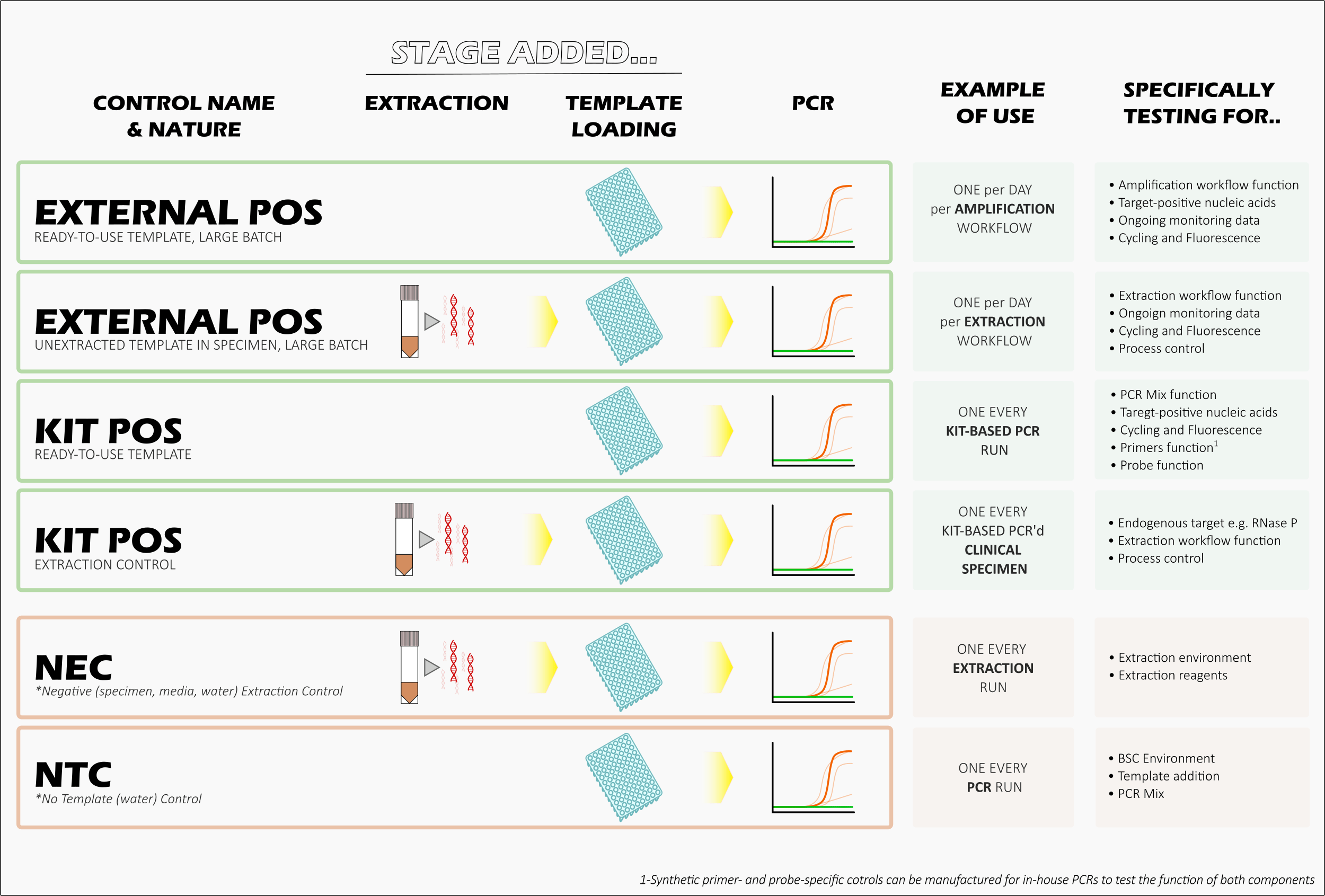
Controls
These must be included in every PCR “run”. These include one known positive and at least one known negative reaction. In these reactions, instead of an extract of patient nucleic acids, you’d add the same volume of known positive or negative material.
You expect these to work. If they don’t, the run’s result should be considered invalid. You then have to troubleshoot the problem and repeat some or all of the patient specimens.
It’s essential to control for contamination of your PCR from the environment where you set up your reaction, the environment where you extract patient nucleic acids from your patient specimen, and the environment where you combine the two. You don’t need to worry about controlling for a post-PCR environment, because in most routine high-throughput pathology labs, you shouldn’t be cracking open a tube after it’s been cycled. 1
In a research environment, there is seldom space to suitably physically separate your PCR steps (a good molecular testing suite requires multiple rooms, a unidirectional workflow and dedicated air-conditioning), so the steps are often performed “on the bench” and quite close to each other. The controls included in research are usually more about ensuring the success of the experiment than the success of the PCR run.2
The process
In place of methods read from grudgingly completed lab books, with or without some tweaks on the day, or a published research paper’s method using almost the exact same ingredients, a pathology lab will usually rely on a single version-controlled and approved ‘IFU’ (Instructions For Use) document that accompanies a commercial PCR kit for each target of interest.3 This provides the method, along with other information, including how to prepare specimens. There will also be commercial nucleic acid extraction methods (another IFU), rather than the more hands-on, low-throughput methods used in the research environment.
Here’s a link to an example IFU for one of MANY different SARS-CoV-2 RT-PCR kits: https://www.bgi.com/wp-content/uploads/sites/2/2021/04/EUA200034-S003.Instructions-for-Use.03292021.pdf
Standardising the whole process is, once again, all about quality and generating a trustworthy result.
Buying a kit means you have paid for the guarantee of quality-controlled ingredients; tested primers, probes and methods; timely delivery of cold-chain-monitored, planned kit quantities; pre-evaluated test sensitivity when used as the company sets out; checking the most appropriate specimen types to test; knowing the PCR cycling conditions program into the thermal cycler; which other targets have been evaluated so we have validated proof that the test only detects what it says it does.
Sometimes the IFU lists the specific instruments that work with the test, because not all ‘PCR machines’ (thermal cyclers) and nucleic acid extraction platforms are the same. Some kits are intended for use on a single analyser (a large, beeping-and-blinking specimen-handling, nucleic acid extraction, and PCR amplification robot). These dedicated kits work only with that instrument and must be used in accordance with the instructions; otherwise, the results are no longer considered suitable for the company to support the lab when it uses its kit.
Cycle numbers
The number of cycles for which we run our PCR is specified in the kit’s IFU. It’s based on past PCR studies. The maximum cycle number may also be locked into an analyser’s operating system. This value is not the same as the threshold cycle (CT).
They will almost always be higher than needed to get a positive result (>40). This high number ensures the Doctor receives all the information they need about how strongly positive the result is.4 The same high cycling number is used in non-commercial PCRs.
It may be important to detect a very small amount of the pathogen, for example, to capture the early stages of an infection in a patient in quarantine. Or to use all the sensitivity of the available tool to be confident that no pathogen traces remain in a patient before their release from an isolation ward after an infection.
Sometimes it’s hard to obtain a negative result. For example, non-specific 16S or 18S PCRs can often highlight the widespread presence of bacterial and fungal DNA, even in commercial reagents. As a result, a ‘cap’ may be put on the results – for example, any result that falls after 28 cycles may be considered irrelevant to a clinical setting. Yes, the target is there, but if it’s not screamingly positive, it may simply be ‘background’ material.
Result interpretation
As above, a positive PCR result may be only one part of a patient’s diagnosis. Some results may require careful contextual interpretation.
Most PCR tests don’t tell you whether the target is replicating or infectious. It usually is. Detectable pathogen nucleic acids don’t appear by magic. Nonetheless, this concept may be noted in the final result report.
The lab is also tasked with ensuring the result is expected. Unlike in research, where you often deal with something you know will be there and often in copious amounts, a patient receiving a diagnosis of infection may rely heavily on PCR results in the absence of other lab evidence.
Monitoring the performance of the PCR run, its controls, other positives and negatives in that run, and the CT values all contribute to the result reported to the Doctor. Sometimes this may need a phone call as well! The report may also specify that a negative result is subject to the nature, timing, volume received or quality of the specimen, or the presence of PCR-inhibitory substances.
Also, without a lot of extra work and specific approaches, PCR is not quantitative on its own, so it doesn’t tell you exactly how much of the target is present. You can’t look at a number and conclude much more than ‘Detected’ or ‘Not Detected’.
Quality
Quality is a major topic in pathology labs, but not as much in many research settings. Quality Control (QC), Quality Assurance (QA), internal quality, external quality, and the Management of all that quality are just next-level in a well-functioning human specimen testing environment.
The brain-dump image below lists key considerations in Quality (inner circle) and the more specific ways they can be addressed (outer circle). It’s worth noting that this includes consideration of the staff and documentation, not just the equipment and reagents used in the test and the testing. Staff expertise, communication, and satisfaction are essential to a well-functioning lab. As well as daily cleaning and resetting of the lab and its equipment, and the thorough logging of those duties.

It’s essential to think about Quality when you are in the midst of it. Quality easily leads to a mountain of physical and digital paperwork that seems like wasted effort. But conducting quality work – work that can be trusted by a lab’s clients – requires traceable documentation. And quality work is essential when the speciomens just keep on mcoming, day upon day upon day.
Poor quality leads to errors which lead to delays which can quickly become incapacitating for a high-throughput pathology lab where rersults mean lives saved and harm reduced. Every result is a patient. One of them could be you.

Quality is about tracking every step and showing that you did. It’s about using standardised methods, and then having all of that checked and audited. Allowing time for that is part of the whole picture. And yes, there is a helluva lot of time involved.
So there you have some key differences between PCR in a pathology lab and its use in a research lab. You’ll know what I mean if you’ve worked in both areas. Hopefully, you know a little bit more than you did at the top of this page, even if you haven’t worked in either!🙂
Exceptions.
- You can perform post-PCR analyses in a PCR suite, but you’ll need extra quality and control measures in that environment. It should be in a separate area, with a process that excludes the user from setting up PCRs until you’ve been home, showered, and changed (= the next day). The post-amplification area is considered “dirty” – filthy is probably a better term – because it may be loaded with PCR product that could get back into your mixes and contaminate the results, leading to false positives.
- This post is filled with averages and generalisations. Of course, your research lab is the most quality-controlled in the world, and, of course, you do everything right. 🙂 But you are not the average.
- Home-brew or in-house PCR methods can also be used in pathology labs, but they require a lot of control to make up for what’s lost by the commercial provision of tidy little white boxes and coloured tubes. But that can absolutely be achieved.
- Almost always, the numerical value (called the cycle threshold, or CT) of a positive result is intended only as a very general indication of how strongly positive the specimen is. There are many reasons not to directly compare CT values between kits, labs, machines, days, or runs, and some of them were covered in The ‘false-positive PCR’ problem is not a problem.
Discover more from Virology Down Under
Subscribe to get the latest posts sent to your email.